Of course, there are decent examples of systems based on primary care such as the NHS of the United Kingdom or Just Kaiser permanent or the Native Health Association of Alaska Slope. But for most Americans, that’s the fantasy land. Instead, we have a system where primary care is the ugly stepson. It is strangling slowly and separates. Only Walmart’s wealth could not make it work.
There are at least 3 types of primary care that have emerged around the last decades. And none of them are very successful in making the idea of ”primary care such as the linchpin of the health of the population.”
The first is the primary care doctor bought by and/or working for the big system. The objective of these practices is to ensure that references for expectations enter the correct hospital system. For a long time, primary care doctors have bones that lose their money money employers said $ 150-250K a year by doctor at the end of the 2000s. So why do they keep them the biggest systems? Because patients who admit in the hospital are incredibly profitable. Consider this NC system that ended in the great atrium of the hospital system because I just wanted references. As expected, the benefits of “cost savings” of primary care are difficult to find among those systems. (If you have time, watch Eric Bricker’s video in Atrium and Troyon/Mecklenberg)
The second is urgent attention. Urgent attention has replaced primary care in much of America. The number of urgent care centers doubled in the last decade more or less. While it has pressure tasks in emergency rooms, URgent Care has replaced primary care because it is convenient and can obtain easy quotes. But he is not doing health management and population care. And of urgent care centers are owned by hospital systems that use them to generate private capital references or pirates that try to increase costs, not control them.
Third, Telesalud, especially attached to pharmacies, has allowed many people to get access to medicines in a cheaper and more convenient way. Of course, this is not really a really complete primary care, but Hims & Hers and their many, many competitors are allowing access to common antibiotics for urinary infections, contraceptive pills and also medications for mental health, as well as those erection and baldness pills.
That does not mean that there are port attempts to build new types of primary care.
Oak Street, Chenmed and Iora (now part of a doctor) were built with the idea of increasing the primary care services given to older people in Medicare Advantage, with the idea that, like Kaiser and their pitos, they take care of themselves. Be careful. Be careful. Be careful. Be careful. Be careful. Be careful. Be careful. Taking to specify can be careful. Taking to specify can be careful. The theory, as always said the founder of Iora Rushika Fernandopulle, was “to double the expense in primary care and reduce general costs by 30%.” It is not too clear if they ever got there.
Of course, like everything else in American Health Care Oak Street and Iora were repetitions of previous efforts of Mullikin, friendly hills, health partners and many more to manage the general costs of care when assuming the risk capted of primary care. None of these experiments were alone for finance brothers enough to see what would have happened if they developed. The stock market of the 1990s and 2020 is full of cemeteries of primary care groups that are quoted in the stock market that had very promising beginnings. If the leg had left only enough time to grow organically, we may see a different future. We could even see that future if it includes health, Transcarent and others manage to build their Primary Care Offering/Telesalud/Navigation/Centers of Excellence. But it’s going to take time
In general, the primary care that carries risks remains a lonely business despite being the preferred policy Wonk solution since Sydney Garfield began the early payment of workers in the Grand Coulee dam in 1933 in 1933
Or of course, this is the United States, you can still get excellent primary care, it will only cost you.
Silicon Valley multimillionaires pay the private year of $ 40ka by Jordan Shlain for the white glove service. At the other end of the scale, a doctor raises $ 80-200 per year of patients who pay for access to the events of the next day, the NP that respond the emails and a free telesalud service for urgent care. In the middle, a large number of doctors who have opted for the discomfort of billing insurers and are charging between $ 500 and $ 5000 a year for concierge care. Then there is a ton of services based on Primary Care, use Telesalud, home visits and NP, or are combined with clinics on the site in workplaces
That the number of those who provide Marcus Welby’s primary care of Marcus Welby in the community continue to fall.
And it is not too difficult to understand why. The average primary doctor does everything less than their specialized counterparts.
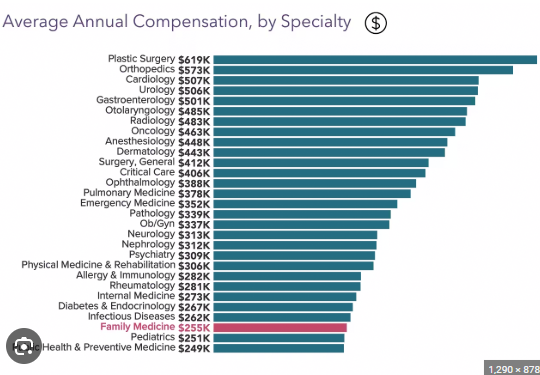
Primary care rates are low. The RUC (the update of the relative value scale) establishes that way, which is dominated by specialists and establishes Medicare rates, which are then followed by most private insurers. Therefore, most doctors tend to look at the upper end of this graphic instead of the bottom that are choosing their residence spaces. American medical attention is expectation because we have too many specialists who have marginally useful attention, and too many hospitals (and pharmaceutical and devices) make the bank out of them. And everything is related to that graph.
Kff was a rather strange count that said that almost 50% of American doctors were in primary care, but that said that many doctors are “primary care” that do not provide primary care. Of course, this is incorrect, but gives a track for the solution.
There are 340 million Americans. We can give everyone a PCP and put them in a panel of 600 people (unlike the 2-3000 typical PCP panel. That number is what MDVIP and other concierge services sacrifice. That would require 570 thoussandcps.
So, if we convert all these PCPs with a current license and add NP, we could give everyone in America in the style of concierge. These doctors would be available immediately and would help their patients navigate the system.
Its defenders believe that concierge medicine is not only better, but also tends to be much cheaper than regular attention. MDVIP states that Salvages $ 2500 per patient just after paying their doctors more, which is about 20% of health spending. My statement is that we could give each PCP $ 2K per patient (or $ 1.2 million per panel of patients with 600), or that they could use (I suppose) $ 300-500K to execute their practice, and could maintain $ 700K to pay.
So, my proposal is that we give all a high -end primary care, they pay very well the primary care documents and save a lot of money. And we apparently have enough primary care documents to do so. Surely if $ 700K was paid a year, we would soon find many more of them.